Our team of data scientists continues to perform analysis on this ongoing global event and its impact on hospitals. We will continue to update the data and visualization(s) in this report to reflect new information.

Executive Summary
To evaluate the financial impact of COVID-19 on U.S. hospitals and health systems, data scientists from Gainfy Network (Gainfy) used a proxy group of related patient cases to model the effect on a representative sample of health systems across the U.S.
Using the model, researchers found that, without raising the reimbursement premium on COVID-19 patient cases, the worst-case scenario will result in 97 percent of health systems losing an average of $2,800 per case, with many losing between $8,000 and $10,000 per case.
Researchers also modeled the results of the proposed 20% increase in Medicare reimbursement for COVID-19 cases contained within the stimulus bill currently under consideration in Congress. Even with this increase, the analysis shows there will be an average loss of about $1,200 per case and up to $6,000 to $8,000 per case for some hospital systems, depending on their payer mix.
Methodology
Gainfy reviewed research from Italy, China and the US Centers for Disease Control before selecting a proxy patient group to simulate the characteristics of COVID-19 patients. Patients were selected from 32 US health systems representing 127 hospitals with 1.2 million combined annual discharges (2019) and $45 billion in annual operational expenses—a subset of the company’s GainfySphere data-sharing network and platform. Patients selected for the proxy group were those who matched the eight DRGs reflecting similar conditions and complications to COVID-19, including pneumonia, respiratory infections, acute respiratory distress syndrome (ARDS), sepsis, and ECMO life support. The cost and payment metrics for these cases were adjusted based on the observed severity of COVID-19, including a 25% addition to total costs.
To model the financial impact, researchers assumed that the 32 institutions would operate at 110% of normal capacity to handle the surge and treat 225,000 COVID-19 patients over the course of 30 days.
While COVID-19 cases tend to skew toward Medicare patients (65 years and older), researchers used mean reimbursement across all payer types for each institution studied, including commercial insurance. As a result, the model may actually underestimate the magnitude of negative margin from these cases.
COVID-19 cases driving unusually high costs
Costs for COVID-19 patients are significantly higher even than their proxy DRG counterparts. The complexity of the patients is causing a decline in nurse staffing ratios as nurses and staff are required to help each other validate that their personal protective equipment (PPE) is properly fitted. Costs are also higher due to expanded cleaning regimens, PPE shortages, more frequent X-rays and CT scans, and overall higher supply and drug costs. Overall, it takes longer and requires more to care for these patients than even the proxy DRGs selected.
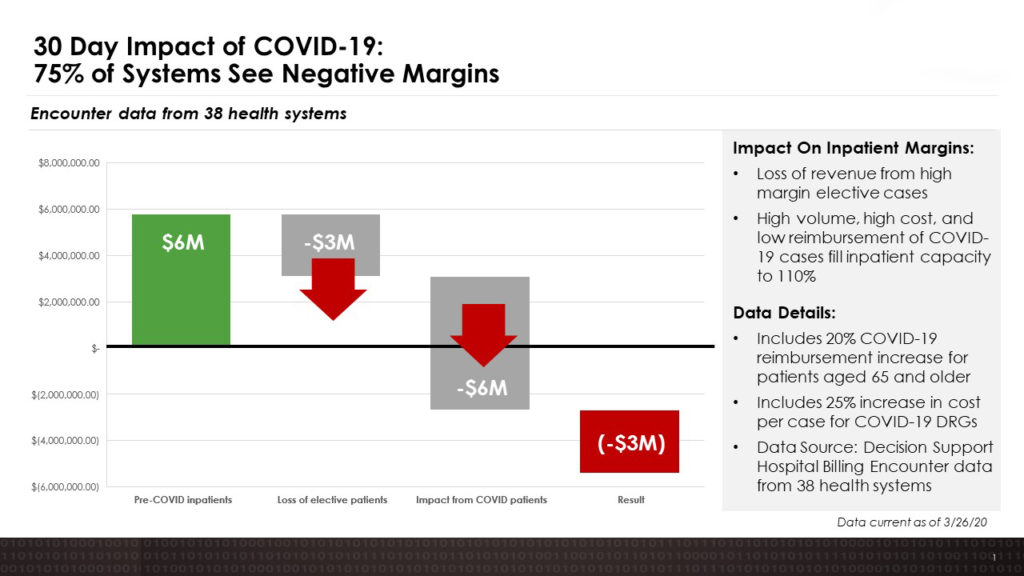
Loss of elective cases prevents cost shifting
Alongside the higher cost of treatment for COVID-19 patients, the model included projected revenue and margin lost from “elective” inpatient services deferred as hospitals make room for more COVID-19 patients. Elective cases are the primary source of revenue for many hospitals, allowing them to take a loss on certain other services while remaining profitable. Researchers estimate that 90% of hospitals that cancel all elective procedures will shortly begin to experience negative profit margins from COVID-19 cases.
Conclusion and Recommendation
With the predicted loss of up to $6,000 to $8,000 per case on treatment of COVID-19 patients, even with the proposed 20% increase in payment, many hospitals will not be able to survive the damage to their cash flow for longer than 60-90 days. Without additional financial relief from government or other sources, they will be forced to take decisive action to reduce costs such as dismissing/furloughing large numbers of non-clinical workers who are already overwhelmed converting hospital beds, maintaining equipment, and performing other non-clinical but essential jobs.
To help reduce the impact of higher costs for COVID-19 cases, as an initial step the federal government should provide a 35% increase in Medicare reimbursement for COVID-19-related DRGs. Even that increase in Medicare reimbursement would not solve the broader enterprise problem of lost revenue from cancelled elective procedures. If the pandemic and correlated loss of elective cases continues into the Fall of 2020, increased reimbursement would need to come from commercial payers and Medicaid as well as Medicare.